News Feed › Discussions › Second question for dr. Brown
-
Second question for dr. Brown
Posted by Jnomesh on March 14, 2019 at 12:13 amHi. Me again. Quick question about your surgery with Dof who has posted his her is repair experience with you.
it was noted by Dog and you that not only did he have a direct hernia but you said there was weakeness in the direct space.
Can you talk a little about what surgeons mesh when they use the term weakeness in regards to hernias and hernia repair. When o had my first hernia repair (direct and indirect ) my implanting (mesh) surgeon noted there was weakeness with fat.
However, when I had my mesh removed my explanating surgeon noted that although there was no hernias upon removal (laparoscopic removal) there was some weakeness in the indirect space and weakeness in the femoral area
it seems you mentioned that dog didn’t have a direct hernia but weakeness which you repaired.
can you talk a little bit about the term “weakeness” and how did you repair the weakness in the direct space if there was no actual hernia present?
Did you repair the indirect hernia and in that repair reinforce the direct space (ie with a shouldice or desarda repair which reinforces both area direct and indirect as I understand it ) or did you do two separate repairs? Thanks in advance.Jnomesh replied 7 years, 3 months ago 7 Members · 16 Replies -
16 Replies
-

Dear Jnomesh.
After mesh removal and the reconstruction of the inguinal floor, your abdominal will probably not be as strong as what God originally gave you. Continue to slowly increase your exercise regimen. But listen to your body.
Aerobic exercises are always safe.
If you messure intra abdominal pressures, Coughing, Constipation, BPH, Smoking are the worst offenders.
I think that your risk for a femoral hernia is small.
Best wishes.
Bill Brown MD -
Dear Scaredtodeath.
After a Prue tissue repair your should be able to return to sports about about 8 weeks.
There should be no long term restrictions.
Below is the link to the regimen I advise for most atletes.
Regards.
Bill Brown MDPost-Op Care & Rehabilitation – Sports Hernia Specialist
https://www.sportshernia.com
Sports hernia diagnosis and repair by sports hernia expert Dr. William H. Brown. -
I would let be to hear Dr Browns experience with excercise as well after tissue repair
-
Dr. Brown I was also wondering since you have worked with many athletes for hernias and sports hernia if you can address exercise specifically weight lifting and running as they pertain tojernkas and the hernia areas.
Dr. Towfigh has mentioned that most exercises Ethan weights are ok and to AVOID excercises that increase intra-abdominal pressure like squats for example. Can you weigh in on this topic?
As I mentioned I had my mesh removed (no hernias present upon removal) after a year of rest I have slowly begun to moderately exercise with weights again. I use a comfortable weight md don’t strain-no squats. Just enough to keep in shape.
Anything I should be doing or NOT doing.
i don’t have any pain after working out. -
Thank you for your response dr. Brown you answers all my questions and your answers were invaluable.
like good intentions I too had my mesh removed-the mesh was implanted laparoscopically for a direct and indirect hernia and removed the same way robotic assisted.
My mesh was found to be balled up into a rock hard ball.
i had it in for 5 years. After removal there were no hernias found as scar tissue brought on ny the mesh scarred in the defects.
Surgeon noted there was some weakeness in the internal ring but he reinforced this while in there laparoscopically by bringing down the internal oblique muscle and seeing it to some other structure. He also found weakeness in the femoral area but said he coold not reinforce laparoscopically Bc this area as it was to vascular.
He said I was st risk in the future of a femoral hernia which is somewhat concerning to me as I had painfully hernias that did not present with a bulge.
like good intentions always in the back of my mind is the possibility of re-herniating in the future even though I am so much better after meh removal and the ordeal it presented.
Since if possible I never want mesh again in the future it’s good to know that open exploratory surgery in the right hands can be done and whatever needs to be repaired (true hernia or weakeness ) can be done so without mesh.
thanks again dr. Brown. -
quote DrBrown:Dear Jnomesh .
When I used the term weakness, I usually mean that the inguinal floor is very thin and if it gets much thinner a direct hernia will result. This is also a very common finding in athletes with sports hernias. Athletes with sports hernia also have injuries to the medial attachment of the inguinal ligament, injuries to the origin of the adductor longus, and osteitis pubis.
Weakness of the inguinal floor often feels just like a direct hernia. Pain and weakness with exercise. Minimal symptoms at rest. But usually no bulge.Hello Dr. Brown. Your response makes me wonder if the damage from mesh implantation and its removal could also lead to a weakened inguinal floor. I’m finding, a year and four months since having two large pieces of TEP implanted Bard Soft Mesh removed that, after rigorous activity or exercise, I still get irritation around the canal, with a feeling of fluid buildup, the feeling of material moving through the bowel, pain and irritation, swelling and pressure. It resolves after a few days of rest but seems to have the signs of a hernia. I had the mesh inside for three active and painful years.
On my hopeful days I convince myself that it’s damaged tissue restructuring and it will slowly get better.
On my most objective and realistic days I think that both inguinal canals are damaged now and that it will never get better and will eventually get worse.
I am still not back to being able to go for a simple run or a gym workout without having pain afterward. I can work, sitting or physical activity, at a reasonable level but I feel like I could be much better off if my abdomen and groins were more healthy.
What is your experience with people that you’ve removed mesh from? I wonder what an exploratory surgery would find, and if it could be improved.
Thank you for sharing your experience.
[USER=”2580″]DrBrown[/USER]
-
Dear Jnomesh .
You are correct. A long standing indirect hernia can stretch the inguinal floor and result in weakness and/or a direct hernia.
The reverse does not occur.
When I used the term weakness, I usually mean that the inguinal floor is very thin and if it gets much thinner a direct hernia will result. This is also a very common finding in athletes with sports hernias. Athletes with sports hernia also have injuries to the medial attachment of the inguinal ligament, injuries to the origin of the adductor longus, and osteitis pubis.
Weakness of the inguinal floor often feels just like a direct hernia. Pain and weakness with exercise. Minimal symptoms at rest. But usually no bulge.
A indirect hernia will have a hernia sac that starts lateral to the inguinal floor and will travel inside the spermatic cord. This sac needs to be separated from the cord and either ligated or inverted into the peritoneum with a purse string suture. If the floor has been weakened from the indirect hernia then a Bassini, Shouldice, or Desarda can fix the weakness. But if the indirect hernia has not weakened the floor then the Marcy Operation is very effective.
A groin exploration will not increase the risk for a hernia in the future.
I hope I answered all your questions.
Regards.
Bill Brown MD -
Dear Chaunce1234,
Bassini was used to reinforce the inguinal floor. A Shouldice would also have been effective. If Dog had had a complete tear the same operation would have been effective.
Both the Bassini and the Shouldice sew the transversalis to the inguinal ligament. But a femoral hernia passes underneath the inguinal ligament and over cooper’s ligament. Thus neither a Bassini nor a Shouldice will fix a femoral hernia. The McVay sews the transversalis to Cooper’s ligament, so it will fix both a direct hernia and femoral hernia.
Regards.
Bill Brown MD -
Wow. I would like to echo the others and say thank you for sharing this and breaking it down in layman terms-ofcoirse l too have some follow up questions:
1) if I’m understanding you right this is the first time I’ve heard that a indirect hernia can potentially lead to a direct hernia as you stated since dog had his indirect hernia for some time it had compromised the muscles causing weakeness in the direct space (although no official hernia).
let me know if I have this right that a indirect hernia could potentially cause a direct hernia and is the opposite true too-that is a direct hernia could weaken the muscles of the area in the indirect hernia space? I have a feeling the second may not be true as a direct hernia is a weakening of the muscles and the indirect hernia has to do with a opening that is there from child birth.
2) is the term weakeness as it pertains to inguinal hernias therefore more associated with the muscles of a direct hernias and maybe a femoral area (hernias ) or would it also include indirect hernias (areas)-in other words all hernia areas
3) from your experience what are some of the most common symptoms someone with weakeness in the direct space be experiencing if there isn’t a hernia if any? Would it be pressure feeling, pain, burning, issues with sitting as the abdominal pressure increases with sitting, or most likely nothing as a hernia hasn’t formed yet
3) would the weakeness of the direct space be synonymous with a sports hernia or is the entirely something different and a different area?
4) it sounds like (but I may be mistaken ) that you did 2 repairs. One for the indirect hernia and the other to strengthen the direct area? Or did suturing the transvasalis Facia to the inguinal ligament take care of both objectives?
does the shouldice and or desarda repairs fix and strengthen both direct and indirect areas in one operation? In other words if one has a indirect hernia and has the shouldice or desarda technique to repair will the direct space automatically become reinforced and stronger even if there is no hernia? And vice versa? Will a direct hernia repair using the shouldice or desarda approach strengthen the indirect area?
5) and lastly can open groin exploratory surgery be done without weakening the indirect and direct spaces risking future hernias if nothing is found upon open exploration?Thank you so much for your earlier replay and thanks in advance for any insight you can shed to any of these other questions I have. Much appreciated
-
quote DrBrown:Dear Jnomesh.
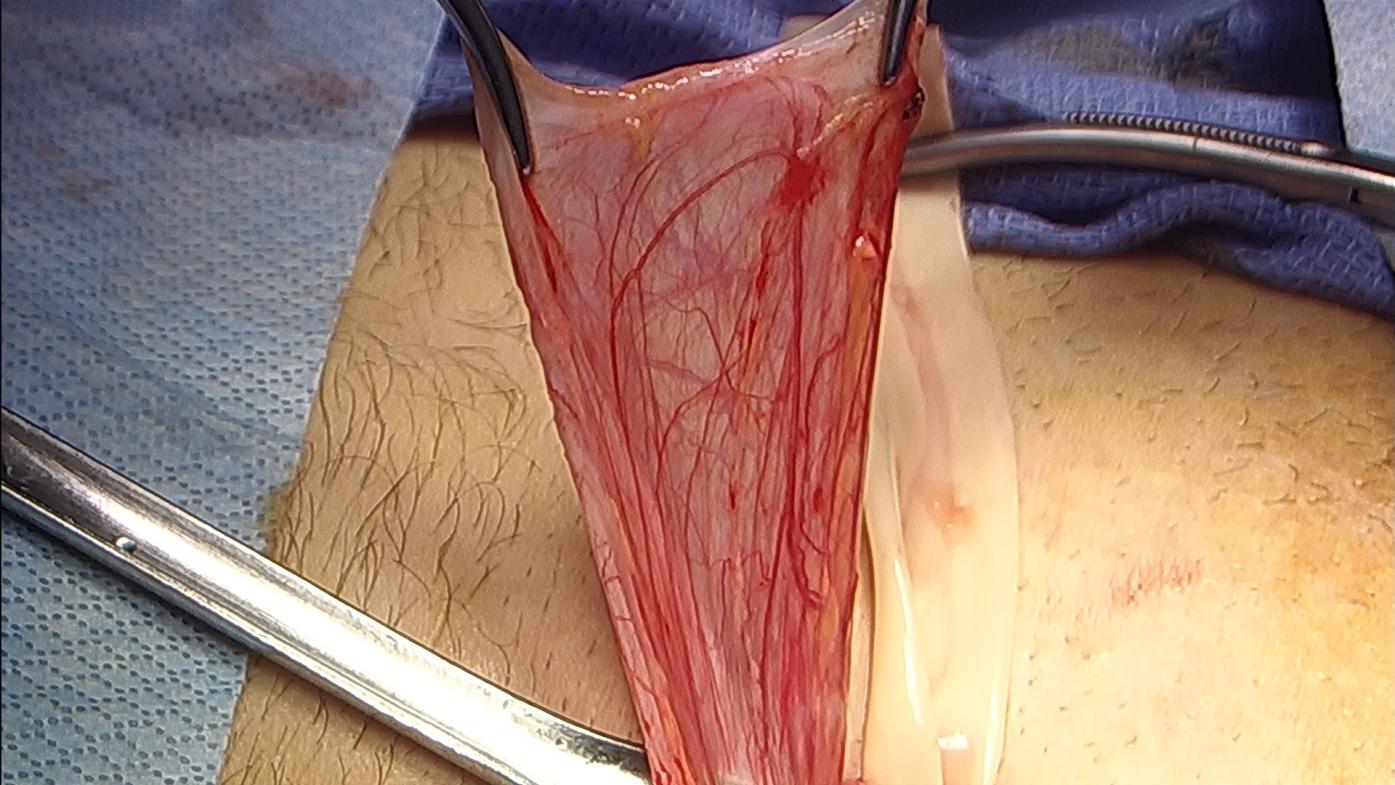
I would like to thank Dog for allowing us to share his photographs.Hernia Sac: this is the sac or balloon that is filled when the intestines pop out through the indirect hernia.
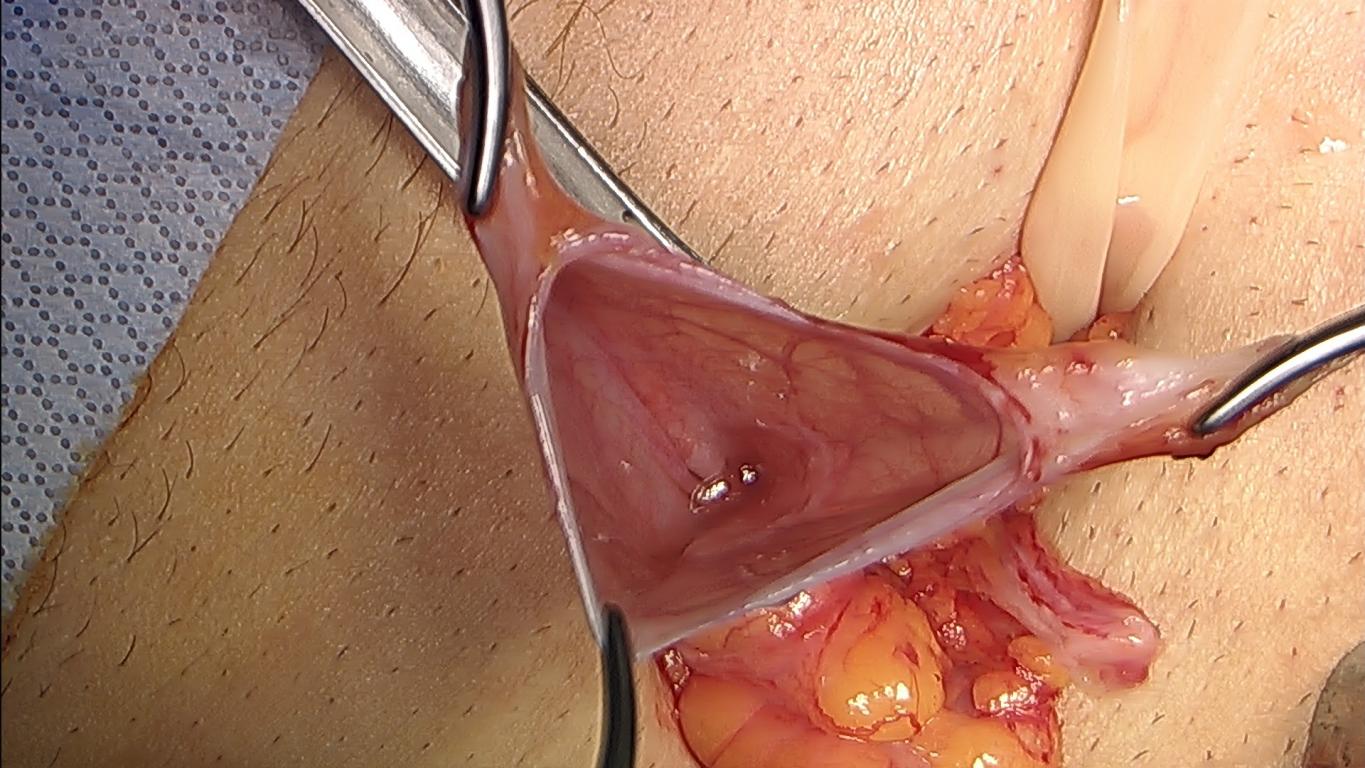
Hernia Sac Opened: In this photo, hernia sac has been cut open and at the very bottom is the hernia. As you can see, even though the hernia sac is large, the actual hernia is small. This is one reason the recurrence rate for indirect hernias is so low.
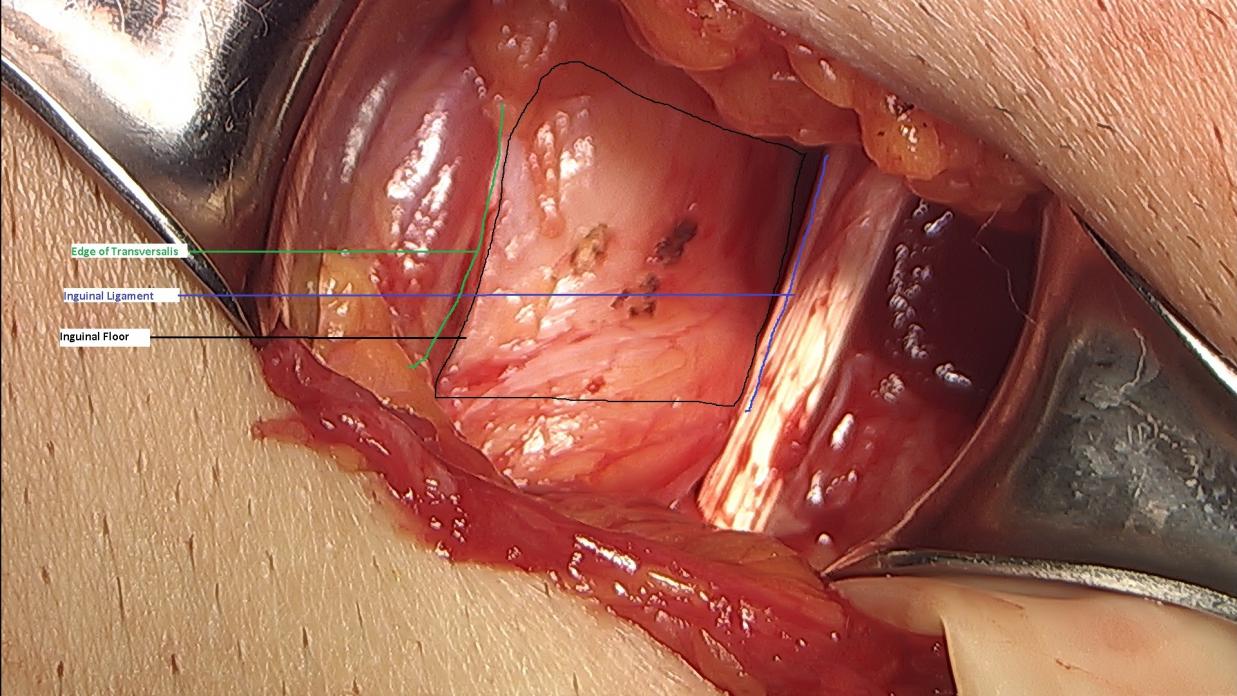
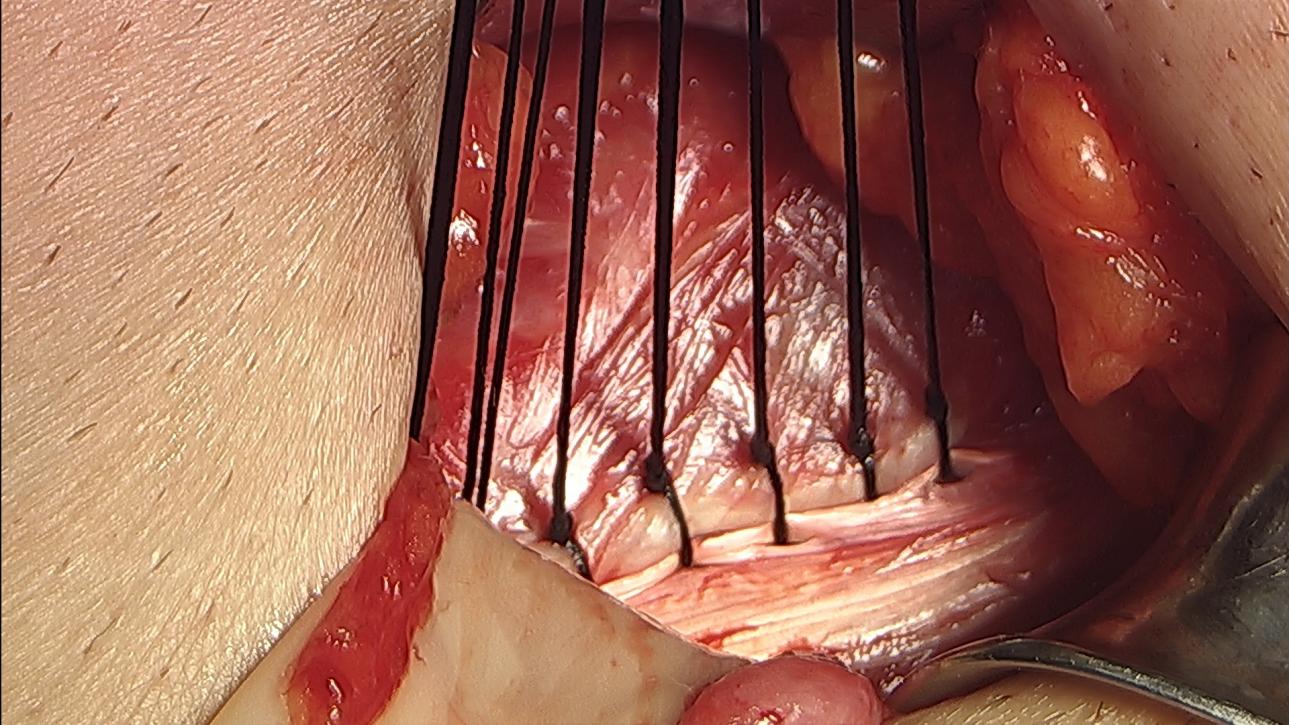
Floor Weakness and Anatomy: Dog had had his hernia for a long time. It had stretched the muscles medial to the indirect hernia. In the photo, notice that the inguinal floor is mostly fat. There is no bulge but there is also no strength. To reconstruct this weakness I will suture the transversalis to the inguinal ligament.
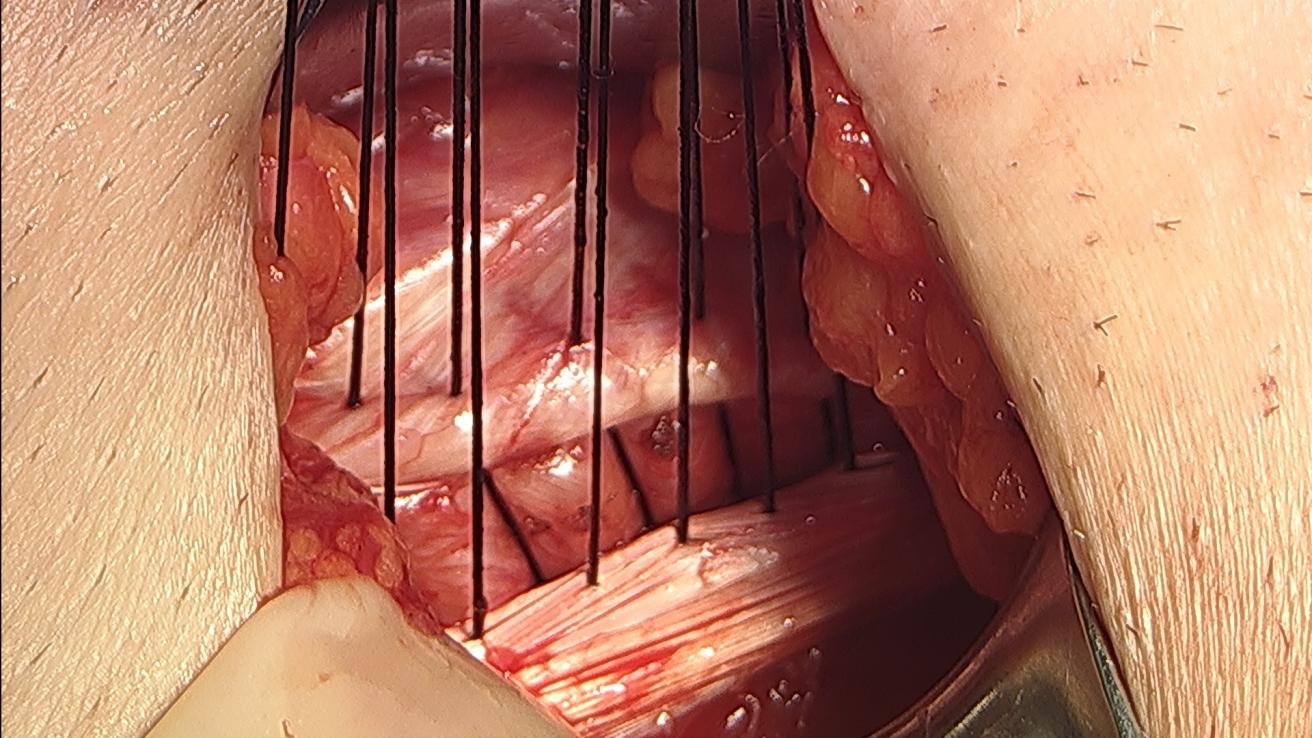
Reinforce Floor: The sutures have been placed between the transversalis and the inguinal ligament.
Repaired Floor: The area of weakness (fatty area) seen in the photo “Floor Weakness and Anatomy” has now been reinforced.I hope that clarifies some of your questions.
Regards.
Bill Brown MDThis is really fascinating even to a laymen like myself, so thank you for sharing these surgical photos [USER=”2580″]DrBrown[/USER] and [USER=”2608″]dog[/USER]
Is this essentially a modified Shouldice or Bassini repair?
If the weakness had torn all the way through the inguinal floor to become a direct hernia, would this still be a suitable repair?
Does this approach also apply to a femoral hernia?
-
Dear Jnomesh.
I would like to thank Dog for allowing us to share his photographs.Hernia Sac: this is the sac or balloon that is filled when the intestines pop out through the indirect hernia.
Hernia Sac Opened: In this photo, hernia sac has been cut open and at the very bottom is the hernia. As you can see, even though the hernia sac is large, the actual hernia is small. This is one reason the recurrence rate for indirect hernias is so low.
Floor Weakness and Anatomy: Dog had had his hernia for a long time. It had stretched the muscles medial to the indirect hernia. In the photo, notice that the inguinal floor is mostly fat. There is no bulge but there is also no strength. To reconstruct this weakness I will suture the transversalis to the inguinal ligament.
Reinforce Floor: The sutures have been placed between the transversalis and the inguinal ligament.
Repaired Floor: The area of weakness (fatty area) seen in the photo “Floor Weakness and Anatomy” has now been reinforced.I hope that clarifies some of your questions.
Regards.
Bill Brown MD
Attachments:
-
Dear Jnomesh.
I have asked Dog if he he will let me post the photos from his operation.
It will clarify many of your questions.
Regards
Bill Brown MD
Log in to reply.