Good intentions
Forum Replies Created
-

Good intentions
MemberMay 10, 2025 at 5:21 pm in reply to: The News Feed page seems to be locked up. No posts allowed. But Discusssions woIt uploaded the image as a document but would not upload it as a picture. Oh well.
The image shows what happens when a person tries to post on the main page.
-
Good intentions
MemberMay 10, 2025 at 5:19 pm in reply to: The News Feed page seems to be locked up. No posts allowed. But Discusssions woI tried to load an image and it failed. Maybe this will work.
-
Realized a minor milestone today. I can wear my old 34 inch waist shorts without pain or discomfort. I had almost given them away since even a 36 inch waist had been uncomfortable. I never thought that my abdomen, the mesh damage zone, would feel right again.
The list of little tricks I developed over the years have all helped. I’ve increased the level of exertion in my exercise and the duration and have taken up running again. The consistent progress, although taking years, shows that it was the mesh that did most of the damage. My abdominal wall seemed to have thickened, and the remnant of mesh that was left behind was still causing pain and localized inflammation. I can still feel it at times but it doesn’t seem to affect as large of an area as it did.
Posting for anyone that is still trying to recover from mesh removal. If things got bad enough to have the mesh removed then the damage that was caused will probably take years to heal and readjust. Don’t lose hope. Just keep working at it. It really is a shame that the community of surgeons has given up trying to find a better hernia repair method.
But the gaslighting, or outright ignorance, continues. It’s pretty amazing.
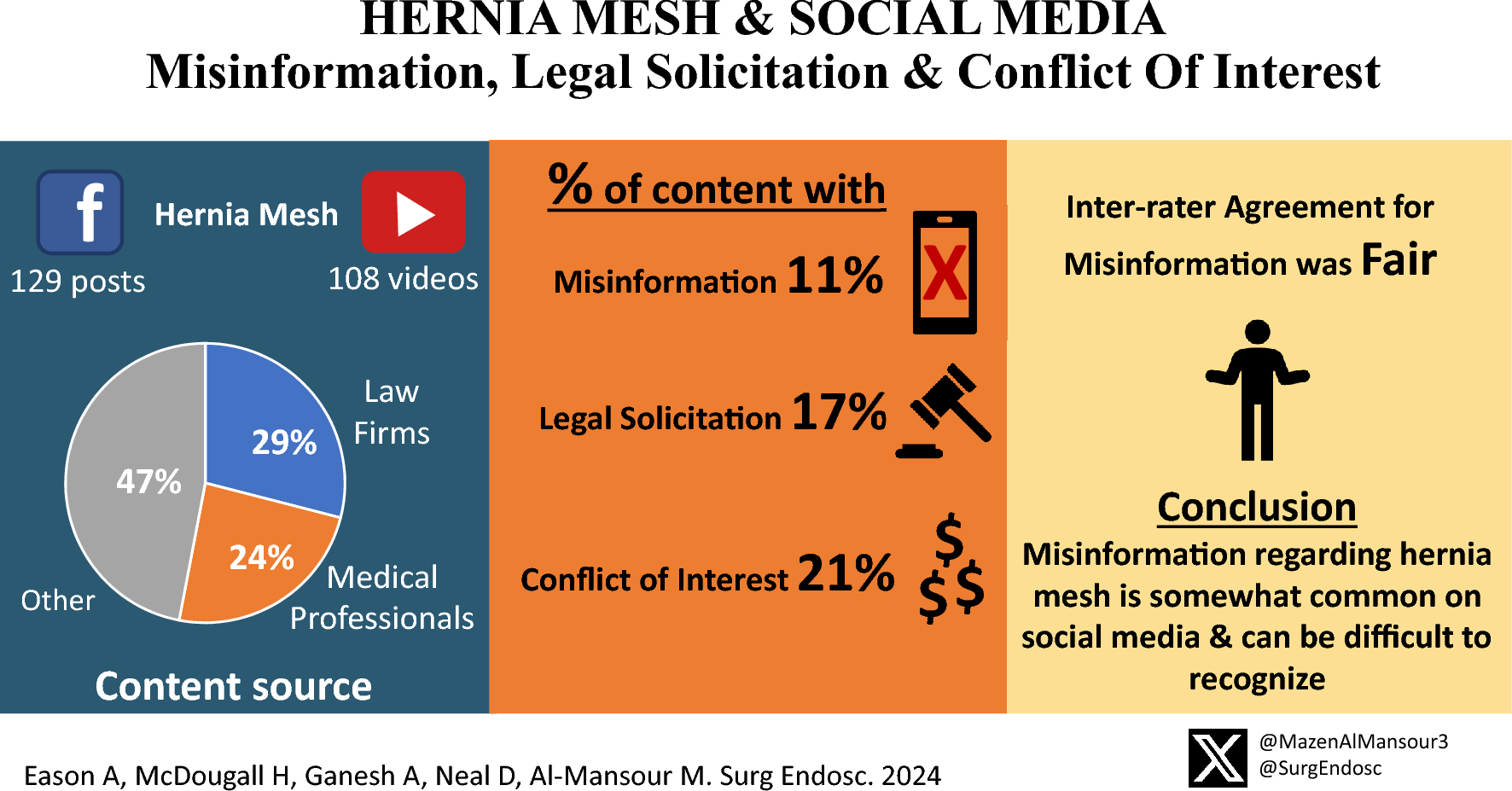
https://link.springer.com/article/10.1007/s00464-024-11320-w
link.springer.com
Background Patients often utilize social media platforms as a resource for medical information. Lately, hernia mesh has been surrounded by controversy due to highly publicized mesh recalls. We aimed to assess the rates of misinformation, legal solicitation, and conflict of … Continue reading
-
https://www.balancedbridge.com/bard-hernia-mesh-2025-updates/
“What does this mean? Again, we cannot know for sure how much the final settlement in the Bard Hernia Mesh MDL is going to total, but with legal fees and the settlement amount, it appears to be near $2 billion.
Something else to know is that this will not be the end of hernia mesh lawsuits. It is unlikely this will even be the end of hernia mesh lawsuits for Bard. Other individuals are still pursuing litigation on their own.
In addition, hernia mesh lawsuits are just now ramping up for other makers of hernia mesh products like Covidien, which now has 1,500 people in its MDL.
The bottom line is, people who have been involved in the long battle of Bard Hernia Mesh products are finally getting close to receiving compensation as the result of their injuries.”
-
It’s been 6 weeks. You’d still be in the mesh/tissue ingrowth and shrinkage phase. Your expectations for immediate return to pain-free action seem way too high but, on the other hand, that is what the typical patient is sold. No surgeon will be doing any surgical procedures on you at just 6 weeks.
And that that space you’re talking about is called the perineum. You’ve probably seen pharma ads about perinum inflammation/pain being a side-effect of various drugs.
Also, it’s pudendal nerve, not pudenal.
Good luck. Wait and don’t overdo things and you might come out okay in the long run.
-
Good intentions
MemberFebruary 9, 2025 at 12:41 pm in reply to: Mesh removal from old open inguinal hernia repairI would see Dr. Kang at the Gibbeum Hospital. in South Korea He removes mesh if needed and will perfrom a pure tissue repair. You can find his posts in the Discussion area of the forum. Use Google to search for them though, the forum software does not work for searching.
http://gibbeum.com/main/main.php
-
Good intentions
MemberJanuary 21, 2025 at 12:55 pm in reply to: The patient perceived as an object, not a personIt’s just surprising that it was not mentioned. As you know, it has been spoken of as the new very significant problem in the field of hernia repair, by the Editor of the Hernia journal, less than two years ago. Other well-known names have called it the #1 problem of hernia repair. Nothing has changed except that now there is a feeling of defeat. Pain after hernia surgery is normal now.
https://link.springer.com/article/10.1007/s10029-022-02576-z
link.springer.com
Chronic pain after inguinal hernia repair is a real risk and a major issue - Hernia
Chronic pain after inguinal hernia repair is a real risk and a major issue - Hernia
-
Good intentions
MemberJanuary 21, 2025 at 12:46 pm in reply to: Hernia repair pain – 5.5 weeks post – doc said location is unusualWhere is the pain in relation to the entry ports? Robotic surgery requires opening the peritoneum from inside, if TAPP is performed, or via splitting the peritoneum away from the wall through the navel if TEP is used. With TAPP the space created needs to be big enough to place the mesh between the peritoneum and the abdominal wall, then it is sewed or stapled shut. Adhesions can occur at the suture line if the sutures are loose.
With the TEP approach sometimes the peritoneum is accidentally torn during blunt dissection (peeling) and needs to be repaired. There might be a suture in the peritoneum at that point.
Your surgery notes will tell you more about what actually happened during your procedure and how big the piece of mesh used was. Some doctors use the biggest piece that they can under the assumption that it will help avoid recurrence after shrinkage. Recurrence is still the greatest fear for the hernia repair surgeon. Pain is somebody else’s problem. Did your surgeon suggest a referral to a different doctor?
Regardless, once the mesh is fully entangled with new tissue there’s not much to be done except hope. 5 1/2 weeks is still early for healing, the body is still encapsulating the fibers of the mesh, but late as far as entanglement and shrinkage. You probably noticed a flattening and tightness of the mesh area after 2-3 weeks. That’s the new tissue grabbing on to the mesh and pulling it inward.
Keep moving, I found that there seemed to be painful areas that were helped by more vigorous movement. I assume that the disruption of fluid supply after surgery and healing caused a poor environment for the nerves in the area. Dr. Bendavid has published about this as a possibility for chronic pain.
Your surgeon is just tossing out ideas, be careful. It’s very simplistic to suggest nerve blocks when pain is involved. Nerve blocks and neurectomy have their own side effects. If nerve blocks work but the pain comes back the next suggestion would be cutting of the nerves, neurectomy.
Good luck. Get your surgery notes.
-
Good intentions
MemberJanuary 3, 2025 at 10:31 am in reply to: Inguinal Hernia repair surgeons in VA or NCIn today’s world “best” often means highest throughput. That’s what healthcare is focused on.
If you can, you might try to contact Dr. Heniford or Dr. Matthews at Atrium Health. They are both aware of the problems with mesh and not afraid to acknowledge them. They’ve been on the hernia meeting presentation circuit. They might have some good advice.
https://atriumhealth.org/for-providers/brent-matthews
https://atriumhealth.org/for-providers/todd-heniford
atriumhealth.org
Brent D. Matthews, MD | Department of Surgery | Atrium Health
Brent D. Matthews, MD, chair of the Department of Surgery at Atrium Health, pursues the innovative frontiers of minimally invasive surgery.
-
Good intentions
MemberFebruary 24, 2025 at 6:35 pm in reply to: Argentine footballer has inguinal hernia repairedI had most of two pieces of Bard SoftMesh removed in late 2017. It was originally implanted in late 2014 for repair of a right-side direct hernia. The surgeon said that he found something on the left side so he did it also. It’s not uncommon, bilateral mesh implantation is popular in the hernia repair field.
A small piece of mesh was left behind on the right side during explantation because it was too entangled with the critical structures of the spermatic cord. It has been an irritant for years, sometimes severe, but has become more of just a mild annoyance over the last couple of years. Sometimes I feel very good and healthy, other times I feel the soreness of the mesh irritation and re-realize that I have not returned to full health. I still carry some of the burden of mesh-based hernia repair.
You can follow the publications in Hernia Journal and see that very little progress has been made in solving the problems with mesh. New studies of the same old problems. The materials have not changed at all.
Here is a new study of fixation methods. The information available to the surgeons to make better decisions is poor. And access to data is typically hidden behind a paywall.
https://link.springer.com/article/10.1007/s10029-025-03276-0
Hernia Article
Mesh fixation in laparoscopic groin hernia repair: a comprehensive review of techniques and devices
Review
Published: 19 February 2025
Volume 29, article number 105, (2025)
Patricia Rancke-Madsen, Stina Öberg & Jacob Rosenberg
Purpose
Laparoscopic groin hernia repair has increased in popularity in recent years. Many laparoscopic mesh fixation techniques and devices are available, but there is a lack of high-certainty evidence favoring one fixation technique over another. This narrative review aimed to provide a comprehensive summary detailing the available mesh fixation techniques and devices used in laparoscopic groin hernia repair.
link.springer.com
Purpose Laparoscopic groin hernia repair has increased in popularity in recent years. Many laparoscopic mesh fixation techniques and devices are available, but there is a lack of high-certainty evidence favoring one fixation technique over another. This narrative review aimed to … Continue reading
-
Good intentions
MemberFebruary 22, 2025 at 11:46 am in reply to: Argentine footballer has inguinal hernia repairedHe is looking very good in the Premier League. Wish we could find out who did his surgery.
-
Good intentions
MemberFebruary 11, 2025 at 1:16 pm in reply to: Mesh removal from old open inguinal hernia repairDr. Peter Billing of Transform Weight Loss removed the mesh in me after it had been in for three years. He does not advertise as a hernia repair or mesh removal surgeon but he has gained a following for mesh removal through word of mouth. He seems to be just a very capable surgeon who understands anatomy and takes the time and effort to get the mesh out with minimal extra damage. I would see him again if I was in the same situation. I have had no regrets about the mesh removal or choice of him as surgeon. It’s been over seven years. Healing from mesh removal does take a long time though. So plan ahead.
He is in Kirkland, WA.
https://www.transformweightloss.com/meet-our-team/
transformweightloss.com
Meet Our Team - Transform Weight Loss
Meet our Team Transform Weight Loss is a weight loss center designed to help our patients and clients achieve and maintain their weight loss goals. Founded by renowned weight loss specialist Peter Billing, MD, FACS, we offer personalized weight loss … Continue reading
-
Good intentions
MemberJanuary 21, 2025 at 2:18 pm in reply to: Hernia repair pain – 5.5 weeks post – doc said location is unusualSorry for the odd order of replies. It’s a glitch of the forum software.
One thing that might help you is to wear clothes that do not put pressure on the painful spot, or cause it to move when you’re walking or sitting. It seems obvious but I have found that the irritation from pressure on my own painful spot would not manifest as pain until afterward. Most pant waistbands cross right over the painful areas created by hernias and hernia surgeries.
I’ve also found that keeping track of activities can help identify correlations. Basically, you have to become hyper-aware of the spot and take care of it, allowing it to heal. It might take months before you get back to your normal routines.
-
Good intentions
MemberJanuary 21, 2025 at 1:42 pm in reply to: Hernia repair pain – 5.5 weeks post – doc said location is unusualSome place like the Cleveland Clinic Chronic Groin Pain Clinic, with Dr. Krpata. He might know enough to head off a problem while it is still small. Link below.
I would still get the surgery notes, even if just for your records. I got mine and sometimes I still wonder if the surgeon who said he did my surgery is actually the one that did it. For his status in the Clinic his notes were surprsingly poor.
5 1/2 weeks is still early. Try to make it work.
https://my.clevelandclinic.org/podcasts/butts-and-guts/chronic-groin-pain-clinic

my.clevelandclinic.org
David Krpata, MD joins Butts and Guts to discuss hernias, chronic groin pain, and treatment options that can bring relief to patients.
-
The mesh lawsuits slowly trudge along. The timing is incredible. Anybody who thinks that they will be “made whole” if things go wrong is completely wrong. Besides the fact that money can never equate to health.
January 8, 2025 – Covidien MDL Moves Forward
The Covidien MDL, which has long been overshadowed by the Bard hernia mesh litigation, continues to make significant progress. Our expectation is that the Covidien cases will ultimately yield higher settlement amounts than the Bard cases, given the scope of the injuries and the design defects alleged in the Covidien products.
Judge M. Page Kelly recently issued Case Management Order 15, outlining a new schedule for key pre-trial activities in 2025. This includes deadlines for general corporate discovery, expert discovery, bellwether trial case selection, and pre-trial motions. These steps will culminate in the first bellwether trials, expected to begin in late 2025 or early 2026. The outcomes of these trials will be critical in shaping settlement negotiations and determining Covidien’s liability.
December 1, 2024 – Closer Look at CMO #55
CMO #55 order establishes the Intensive Settlement Process (ISP) to facilitate the resolution of cases and appoints Ellen K. Reisman and John Jackson as Special Masters to oversee the process. Their duties include supervising settlement negotiations, mediating disputes, and ensuring that the ISP progresses efficiently. The Special Masters will report quarterly to the Court on the ISP’s status.
The ISP is scheduled to begin in January 2027. This is not a typo. If you want to opt-out and settle your claim, you are put on ice for over two years.
Monthly settlement conferences and mediations will then commence to address unresolved claims. Plaintiffs will be required to submit comprehensive settlement packages in advance. If cases are not resolved in the initial conferences, formal mediations will be held under the supervision of a Special Master. Costs for mediations will be evenly divided between Bard and the plaintiffs participating in each session.
The ISP will remain active until all unresolved claims have been addressed, providing an opportunity for plaintiffs to negotiate settlements efficiently. However, if cases remain unresolved by June 2029, claimants may opt out of the process and proceed under the applicable docket control orders. So if you plan is to take your case to trial, the plan is to make you wait for over four-and-a-half years just to get the ball rolling again. Will this leave a lot of plaintiffs very bitter? Yes.
lawsuit-information-center.com
Currently, thousands of hernia mesh lawsuits are pending in courts across the country. Our hernia mesh lawyers are handling these cases in all 50 states. This page: Discusses this litigation ...
-
Good intentions
MemberJanuary 11, 2025 at 4:36 pm in reply to: Anybody in BC, Canada, with inguinal hernia? Surgeons/procedure you recommend?Dr. Ondiveeran, shown in your link, would be worth seeking out. He seems very open-minded, rational and independent-thinking. Most surgeons just do what they are instructed to do by their clinic or hospital supervisors. And mesh is the mainstream repair method today, it is faster and more cost-effective for the institutions.
Dr. Jacob is quoted also and illustrates the mind-set that people who avoid mesh are just getting advice from the inernet. Then gives the “tough luck, it is what it is” view, “they need to be willing to accept that”. Kind of protective of the status quo.
It’s from 2017, back when their was a big push to understand the problems. Unfortunately, little progress was made and things have stayed the same.
Dr. Jacob – ““In New York, some patients come to me having done their own online research and they have decided that they don’t want mesh,” said Brian Jacob, MD, assistant clinical professor of surgery at Mount Sinai Hospital, in New York City, and the owner of nychernia.com. …
Patients need to understand that research has shown that hernia repairs without mesh can have higher recurrence rates and still have some reports of chronic pain, and so they need to be willing to accept that,” Dr. Jacob pointed out. “
…
Dr. Ondiveeran – “Polypropylene reinforcement has been the gold standard since Irving L. Lichtenstein, MD, promoted it in the 1980s. “We are really doing very well with it. Recurrence rates are low, about 2%. But recurrence isn’t the only concern,” said Hari Kumar Ondiveeran, MD, at the 2016 annual meeting of the International Hernia Collaboration.
“What about pain? What about the feeling of discomfort young patients complain about having a foreign material in the groin? What about immune response? Is polypropylene as inert as we think it is? And what about cost?””
-
Good intentions
MemberDecember 10, 2024 at 7:47 pm in reply to: Mesh less repair after 8 month : disasterMaybe he was getting a CT scan with barium sulfate contrast agent. That’s the one you drink.
-
Good intentions
MemberDecember 10, 2024 at 11:07 am in reply to: Argentine footballer has inguinal hernia repairedI would bet that he went to Dr. Muschaweck. She is the surgeon the big clubs use for abdominal surgery.
-
Good intentions
MemberDecember 9, 2024 at 12:10 pm in reply to: Argentine footballer has inguinal hernia repairedHe scored yesterday and seemed pretty happy. Of course, when I had mesh inside I felt good while active. It was the after-effects of physical activity that were intolerable. Time will tell.
-
Delay, delay, delay.
Here’s the latest on the hernia mesh lawsuits. Anybody who thinks that they will have timely recourse for mesh damages is delusional. The law firms and device makers have all of the resources and time to wait people out.
“<b style=”background-color: var(–bb-content-background-color); font-family: inherit; font-size: inherit; color: var(–bb-body-text-color);”>December 2, 2024 Update
A new case management order CMO introduces the Intensive Settlement Process (ISP), a structured framework aimed at resolving cases efficiently by appointing Ellen K. Reisman and John Jackson as Special Masters to oversee its implementation. These Special Masters are tasked with supervising negotiations, mediating disputes, and ensuring timely progress, reporting quarterly to the Court on the ISP’s status.
The time horizon on this will be depressing for many. The process is set to launch in January 2027, requiring plaintiffs to endure a significant delay of over two years before active settlement efforts commence. The ISP will continue until all claims are addressed, but unresolved cases by June 2029 will allow claimants to exit the process and resume litigation under docket control orders. For plaintiffs hoping for a quicker resolution or trial, this extended timeline—at lease four-and-a-half years if Bard’s offer is not nearly where you want to be—will prove deeply frustrating for many victims.”
https://www.lawsuit-information-center.com/bard-hernia-mesh-lawsuits.html
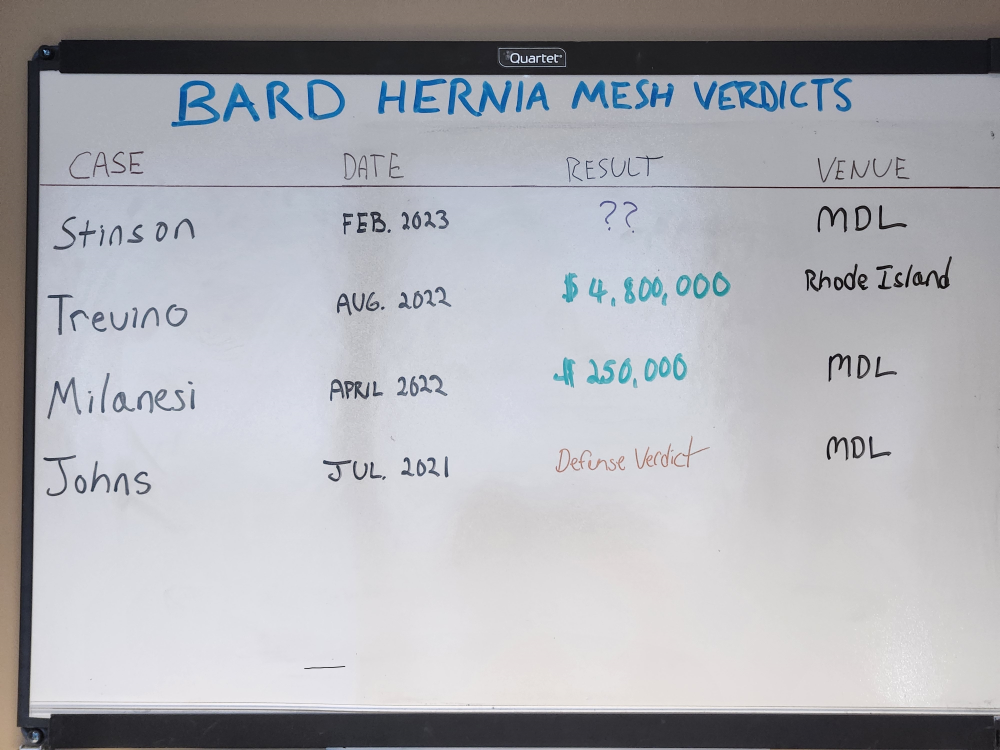
lawsuit-information-center.com
Hernia Mesh Lawsuit Against C.R. Bard
C.R. Bard is defending over 18,000 hernia mesh lawsuits alleging that its mesh devices were defective, resulting in injuries and complications for thousands of hernia surgery patients. Our hernia ...