
Good intentions
Forum Replies Created
-

-
It didn’t work. try this -www dot goremedical.com/sites/g/files/ypyipe626/files/resources/assets/2017-10/AD0205-EN5.DLM_FINAL.pdf
Paste this in to a browser and replace the first “dot” with a period.
-
Here is the second.
-
Here are the links to one the two sources I used.
-
It has tiny pores, of less than three microns, apparently. A typical polypropylene mesh will have pores of about 0.55 to 1.5 mm. Huge compared to the Gore pores. Microns to millimeters.
I will post the links in a second post. The site often locks up my post when I try to add a web link.
Gore has web pages that describe their products, and Dr. Robert Bendavid has summarized the state of polypropylene mesh with pore sizes in some of his publications. Those are my two sources.
-
Good intentions
MemberMarch 21, 2018 at 5:26 am in reply to: Failed bilateral inguinal hernia after 3 monthsnesd, your case is unusual because you have reported a failure of the mesh repair, a recurrence of the hernias. That’s not supposed to happen. But it’s unclear from your first post that any of the three surgeons you saw afterward actually confirmed a failure. You said that they told you what they would do to fix what you told them had happened, but you didn’t say that they confirmed that the prior repair failed. Your description of a “bounce” during the examination is odd also. And the fact that your surgeon said that he would like to get his associate involved makes one wonder if he is unsure about what’s actually happening. It’s also unclear what type your initial hernias were, direct or indirect.
I’m not sure anyone can give good advice beyond “find a surgeon who is known to be knowledgeable in hernia repair”. I reread your first post and there is really not much information about what your actual condition was before the mesh implantation, or what it is now. It doesn’t sound like you are in pain or discomfort so taking the time to understand your true condition would be worthwhile. Unfortunately, apparently, there are doctors ready to accept you as a patient and do what they do, but it’s not clear what you need to have done, to be well again. I would try to learn more about your condition, and get your medical records together so that you can accurately describe what your problem is.
-
Good intentions
MemberMarch 18, 2018 at 6:46 pm in reply to: Comparison of Non-Mesh repair tyes (Desarda, Darn, McVay, Bassini)Hello. I notice that you left out the Shouldice repair method. Also, Dr. Kang and his method, in South Korea.
What type of inguinal hernia do you have? And what type of activities are you hoping to do afterward? Those might be considerations. Good luck.
-
Good intentions
MemberMarch 16, 2018 at 5:56 pm in reply to: Klebsiella pneumoniae found in abdominal abcess mesh removal!!Hello Amanda. I would contact Dr. Towfigh directly by sending her a message. She has experience in working with infected mesh, and has published in the past.
Click her name in the sticky at the top of the main page.
Can you give more detail about the operation. Type/brand or mesh, type of hernia, etc?
Also, the Carolina group works on infected mesh problems.
https://www.carolinashealthcare.org/for-providers/todd-heniford
-
Good intentions
MemberMarch 16, 2018 at 5:54 pm in reply to: Klebsiella pneumoniae found in abdominal abcess mesh removal!!Hello Amanda. Good idea to start a new thread. I have seen past work by Dr. Towfigh dealing with “infected fields” and another type of mesh, biologic mesh. She might have a more direct interest in your husband’s problem, since she has experience with it. You could send her a message using the forum’s messaging function.
Click her name on the sticky at the top of the main page of the forum. You can also contact her work place, there’s a link on the Surgeons page. Or use the links I copied below.
Can you give more details about the operation and the types of mesh? It’s unclear if all meshes cause problems or if specific weave patterns and materials cause problems. There might be a clue in the details. It’s possible that the place that did the original repair in 2008 still has his records, although many institutions purge their files after a relatively short time. It would be worthwhile to contact them and see.
Here are links to the ways to contact Dr Towfigh –
https://www.herniatalk.com/member/935-drtowfigh
https://www.herniatalk.com/surgeons
The Carolinas group also seems to do a lot of work with infected mesh problems.
https://www.youtube.com/watch?v=ri4_afSvGms
https://www.carolinashealthcare.org/for-providers/todd-heniford
-
Good intentions
MemberMarch 16, 2018 at 6:21 am in reply to: Failed bilateral inguinal hernia after 3 monthsI suggest seeing a surgeon who has experience in mesh removal. Because they might have seen the symptoms that you’re describing and will know the signs of mesh rejection. There are hundreds or thousands of surgeon who know how to implant mesh but few that know what to do when it doesn’t work. Dr. Towfigh, Dr. Billing, Dr. Belyansky, and others will remove mesh if it is the cause of your problems.
You also mentioned that the mesh that was implanted is the “self-sticking” type. There are at least two type of “self-sticking” or tackless mesh. You really need to get your medical records so that future doctors know what they are dealing with. That should be your #1 focus – get those medical records. It might be that one or more the new mesh designs isn’t working well.
Many surgeons will work with you via email or phone as an initial consultation. Get your medical records then email, or paper-mail, a descriptive letter and your records out to them. Paper mail if you’re worried about confidentiality. When I had my problems I didn’t care who knew about them but it is something to consider.
Also, don’t assume that any “good” surgeon should be able to help you. It’s the individual surgeons that put the extra time beyond their general medical education that will have the answers. You’re not part of the general population any more. Mesh is supposed to work, always.
Good luck. Don’t despair. There are doctors out there who are willing and able to deal with these problems.
-
Good intentions
MemberMarch 14, 2018 at 3:28 am in reply to: Failed bilateral inguinal hernia after 3 monthsSince you already have mesh implanted you should make careful note of how your body is responding to the mesh itself. If you feel like the area is more inflamed than when you had the hernias then more mesh might be a bad idea. It might solve the hernias but leave you with new problems. Excessive inflammation from mesh is a real problem, but not one that the repair industry wants to deal with.
Take a little more time and get a copy of your medical records from the surgery. There might be some information there that will help a good knowledgeable surgeon, who stays current with what’s happening in the hernia repair field, to figure out why your first surgery failed. It might be that your body is just rejecting the mesh and that it never did “bond” to the muscle wall like it was supposed to do. Just floating in a sea of inflamed tissue, moving in to the original hernia sites. If that’s the case then more mesh would not seem like the solution to your problem.
Try to get more detail about the material and the methods the surgeons that you see propose. There is much more detail available than just “open” or “mesh”. The details are what matter. There many different types of mesh, and device designs, some of them pretty bizarre. And some of them have a history of problems, so you can avoid those if you know they are part of the plan.
Good luck. Most of the doctors that you see will only have experience in implanting their type of mesh, their way. You need to find one with a broad base of experience since you’re outside the norm.
-
Good intentions
MemberMarch 8, 2018 at 5:36 pm in reply to: Painless throbbing years after mesh repairFour years is not that long. Nerve regeneration and growth will continue, probably forever. Even proponents of mesh will acknowledge that the body will be “working” on the mesh as long as it is there, as a foreign body. Whether for good, tissue ingrowth to hold it in place, or bad, constant inflammation. I am aware of at least one person who had some form of mesh implanted many years before a second repair on the other side, and the more recent repair caused problems, while the old repair was fine. The materials and techniques are constantly changing, often for unclear reasons, so what you had done in 2003 might not really be “identical” to what you had in 2014. You haven’t supplied any details beyond “mesh” either. That doesn’t tell much.
Look for Dr. Kang’s posts on this site. He seems to understand the field. He might know somebody that can help. He is based in South Korea.
Here are search results. He hasn’t been active lately but he was very helpful for a short while.
https://www.herniatalk.com/search?q=dr.+kang&searchJSON=%7B“keywords”%3A”dr.+ kang”%7D
Here’s a link about nerve growth – http://file.scirp.org/pdf/IJCM_2014072117033945.pdf
-
I just posted in your other topic.
When choosing a surgeon, and even more importantly, what type of surgery to have to repair your hernia, extend your results time-frame way out to when you are old and feeble. Because that is how long you will be living with the results of your choice. The two weeks or months or even years that of time that you save by making a quick decision will seem like nothing if the results are poor. I know of people who have dealt with poor repair (mesh) problems, for many years. I spent the three immediate years after my surgery dealing with the issue.
See Dr. Towfigh’s recent topic about a Patient Advocacy Forum. https://www.herniatalk.com/6583-dear-patient-advocates-seeking-feedback
Good luck. Don’t assume that the people you see complaining are just outliers, or people who had surgery before the methods and materials were developed. I was strong and healthy and had those thoughts until I became one of them. The same materials and methods have been used for at least the last 12 years and people keep getting screwed up. And the people you see on the internet are just the tip of the iceberg.
Be careful.
-
Good intentions
MemberFebruary 27, 2018 at 3:57 am in reply to: Inguinal hernia and exercise/liftingI recall that post from Dr. Towfigh and as I recall it was referring to studies that others have done. More specifically, I think that she referred to “barbell lifting”, which, of course, is an odd way to refer to weight lifting. I think that it was recent and you could probably find it by browsing topic titles. It was similar to yours, I think.
My understanding of hernias is that once the “hole” is created, it’s abdominal pressure that will push material through it. So you want to avoid things similar to the valsava maneuver, a common weight-lifting technique to stabilize the pelvis, that pressurizes the abdomen. Personally, from my own experience, I would also avoid activities that might result in rapid reactions that create abdominal pressure. I played soccer after my hernia and think that reacting to the situation around me caused the hernia to increase in size. But, just before my repair surgery, I was able to run a couple of easy miles and do easy workouts at the gym. I had the surgery in an attempt to get back to my higher level of activity. It didn’t work.
I saw your other post. There is a lot of good information on this forum. Read carefully and consider well.
-
Good intentions
MemberFebruary 26, 2018 at 6:33 am in reply to: Dear Patient Advocates: Seeking FeedbackThis is exciting Dr. Towfigh. I hope that some good comes from it.
One question I would like to pose, that I’ve also recently posted about, is the extent of the role of the FDA in approving new devices. Of course, mesh is defined as a medical device. Do the medical device makers supply the approval data, or does the FDA do actual product testing? If the FDA does testing, where can the results be found? If the device makers supply the data, how can they be held to account if their data does not match reality? And where can their data be found?
A second question would be – how is adverse event data collected? Who supplies it, and who collects and tabulates it? For example, if I, as a patient, complain to my surgeon that I have a problem with my mesh implant, how far along the path to removal do I have to go before it gets recognized as an adverse event? Is the first complaint the trigger, or does some actual physical action have to take place? Do the doctors and surgeons trust the adverse event reporting function of the FDA? Do they have a professional obligation to report what their patients tell them?
There are many stories about patients who can’t find relief from what they feel are bad mesh reactions, but it’s not clear if the FDA knows about these patients.
I look forward to seeing this effort progress. It might be that small changes could have big effects. But without good information nobody knows what to act on.
-
Good intentions
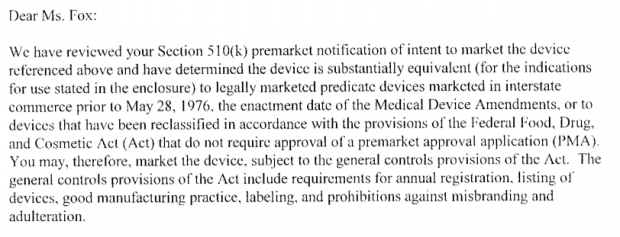
MemberFebruary 26, 2018 at 6:21 am in reply to: Substantially Equivalent – How medical devices can deviateHere is an example of how far back they go for the original material that everything following is equivalent to. The trail of equivalence starts in 1976.
Of course, there are other requirements to meet before selling the product. But the bar seems very low from the start.
-
Good intentions
MemberFebruary 26, 2018 at 3:12 am in reply to: Losing touch with the patient – modern medicineI think that the doctors that are part of bigger practices/clinics have too much paperwork to do to maintain a personal relationship with their patients. Plus, in today’s health care system, they probably have to account for all of their time, and each patient contact. It might also be part of today’s training, to maintain a certain distance from their patients. And, typical of large efforts, division of labor is more prevalent. Specialists that only do a few things, and have to leave other tasks to other specialists. So that the insurance company codes will fit.
I think I know who the sports hernia doctor is. He contacted me quickly also. It was odd and surprising, having been used to the day or more delays after every communication attempt, but after some conversation I realized that he was just being more true to his profession. He is very knowledgable.
I notice that you seem to have decided that you have a sports hernia. I read your story in your other posts and it doesn’t seem like it would be a typical sports hernia. You might be limiting your possibilities.
-
Good intentions
MemberFebruary 26, 2018 at 2:40 am in reply to: Questions re: inguinal hernia repairquote Beenthere:The knowledge, skill and experience have more to do with the outcome than mesh or no mesh.Beenthere, I know that you’ve been through a lot, I’ve read your posts. But this, what you wrote above, is the standard meme being propagated by the medical device makers. I think that many doctors and surgeons actually believe this to be true also. No surgeon wants to think that what they are doing can cause harm. So, it’s easier to believe that it was the fault of an unskilled surgeon, a beginner maybe, not the mesh material itself, that is causing people harm
I think that this is one reason that surgeons are so resistant when their patients come back with problems. It’s just not supposed to be, especially if they are very skilled. They did everything “right”. But some or all of the mesh materials are not “right”. So it won’t matter how skilled the surgeon is, it’s the material that is the problem.
My surgeon was top-notch and actually part of a group that trained and certified fellow surgeons in the latest laparoscopic techniques. It didn’t matter, it was the Bard Soft Mesh itself that caused the problem, via constant inflammation. He did everything by the book.
The industry has a huge investment in the process and the materials. So much so that it’s almost incomprehensible to them that it’s not working the way they thought it was going to. Or, worse, it is known to some, but the business is too good to change anything, Like gun sales. Until a better material is developed, the surgeons will continue forward with what they were trained to do, hoping that stories like mine are total outliers. There will be a constant stream of injured patients, populating forums like this one. And probably many more people who just aren’t harmed enough to seek help, or post on forums like this, but aren’t in the shape that they were promised. Diminished, but still functional. The harm isn’t on/off, black or white, it’s a continuous spectrum.
It’s a terrible situation, with doctors and patients both, and other medical professionals, constantly seeing these mesh inflammation problems. Imagine being in the healing profession and knowing that there’s something wrong with what you’re doing, but having no one to turn to to help figure it out. Only a few people are stepping up to address the reality of what they see, but progress is very slow.
So, please don’t pass on the false memes out there, that a patient just has to find the right surgeon, and that all mesh materials are essentially the same. It’s just not true.
-
Good intentions
MemberFebruary 25, 2018 at 6:31 pm in reply to: Questions re: inguinal hernia repairI had posted a long post, recommending that you consider what you plan to do after the surgery, with other details. Hopefully, it is allowed, I added a link to Ethicon’s web site and it got flagged as possible spam.
Mesh has more problems with active people. If you plan to be physically active, take extra care in what you choose.